




















My Experience on a Ventilator
There is a lot of talk about the need for more ventilators to intubate critical COVID-19 patients. It is called a necessary life-saving piece of equipment. It got me wondering how many people come off intubation to return to a healthy life. It was not only my normal curiosity and desire to delve deeper into factual information, but I can speak from experience – having been intubated a couple of years ago.
I had been experiencing weakness, shakiness, tiredness and occasional light-headedness. I assumed they were just the manifestation of aging. On one occasion I became seriously dizzy and called 911. As they started to work on me, I asked if they could take me to my normal hospital – the Cleveland Clinic in Weston, Florida.
That is when I got my first hint of the seriousness of my condition. They said that had to get me to the hospital as soon as possible – as they put it, my “numbers were not good.” I got my second hint of the danger when the first hospital said that I had to be transferred to the larger Delray Hospital that could better handle my case. I suddenly felt sicker and vomited in the second ambulance ride – which gave me a heightened appreciation of what the emergency personnel have to deal with. They could not have treated me better.
I arrived at the hospital and was immediately taken into the operating room. As I recall they wanted to check out my heart – maybe needed an angioplasty. That is when I lost consciousness.
I began to come around – and to this day cannot recall how long I was out. My biggest problem was that tube down my throat. Every time I swallowed, my larynx would squeeze on the tube. I cannot say it was excruciating pain, but it was such an extreme discomfort that I wanted to pull that damn thing out.
As I came around, I heard the voice of the nurse. “Well, it is our miracle man.” Her job was to sit beside me to prevent me from pulling out the tube. In the kindest of tones, she would say “No. No. You have to leave that in for a while” as she would gently restrain my hand.
Eventually, the tube was removed, and I could communicate cogently with the doctors and the nurses. I was called the miracle man because I was not expected to survive. The doctors were so sure of my imminent demise that they had called my estranged wife to inform her of my pending death. She notified the kids.
As it was explained to me, my blood pressure had collapsed, my kidneys stopped functioning and my heart began racing – which usually ends with heart failure. Fortunately, I have a very strong heart and it did not blow out. The doctors were able to pull me back from the abyss of eternity.
As a postscript, I met a Chinese cardiologist, Dr. Michael Shen, who originally came from Harbin in northern China. By unbelievable coincidence, I had been the foreign investment advisor to the City of Harbin for several years. Dr. Shen and I become instant friends.
He took a special interest in my case and determined that my problem was too much blood pressure medication. He reconfigured all my prescriptions and – you will not believe this – within a week I felt 20 years younger. No more shakes. No more dizziness. After 20 years away from the courts, I returned to playing tennis several times a week and bought a bicycle. I not only survived, I was revitalized. For obvious reasons, Dr. Shen remains my cardiologist and general health advisor.
Based on my own experience and with so much talk about the life-saving importance of ventilators, I decided to do a little research. What I found gave me a much greater appreciation of my own good fortune and yet a more pessimistic impression of the value of the machines. They most certainly do save lives. I am an example. But the ventilators apparently do not save as many lives as you might think.
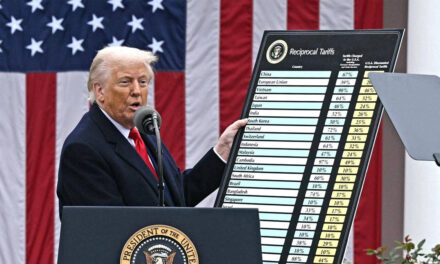
Studies vary widely. The most positive experience reported had a mortality rate for intubated patients of 48 percent. Most studies, however, showed a much higher death rate. In some situations, the rate has been as high as 97 percent.
According to a Physicians Weekly article, a Chinese study of 22 critical care patients who were put on ventilators resulted in 19 (86%) dying. In another study, 31 out of 32 ventilated patients died (97%). In a British study, 66 percent of patients on ventilators did not survive.
Another problem with intubation is that even with patients who survive, the procedure itself can produce temporary or permanent damage – with the likelihood increasing the longer a patient remains intubated. A long-term patient may not be able to breathe naturally ever again. In that case, a tracheostomy would be required to implant a permanent breathing tube.
The press is filled with speculative reports of having two critically ill patients and only one ventilator – a Hobson’s choice. It can be a heart-wrenching choice. But based on the data, it is unfortunately more likely that both patients would die. By the time a person needs to be intubated, the future outcome is not hopeful. This is particularly true if the patient is older, critically ill and already has underlying conditions.
The COVID-19 virus will cause the death of tens of thousands of mostly older Americans, but the lack of a ventilator may not be the issue. Fortunately, up to now, we have had enough ventilators available to those needing them – and it appears that the ginned-up ventilator crisis did not happen and will not.
In my own experience, I was more than lucky. I survived. I was off the ventilator quickly – and had no negative aftereffects. I came out of it better than ever – mainly because I was healthy and without any underlying pulmonary problems. I was not weakened by sickness. I was improperly medicated – a problem that was easily fixed by a very caring and competent doctor.
So, there ‘tis.




Like Chemotherapy to treat cancer, more people died because of Chemotherapy than survive.
I have no doubt ventilators are valuable medical devices. But by virtue(?) of their intrusiveness in the most delicate areas of the body, they are also extremely dangerous. The mortality stats Larry cites are mute testimony to their dangers.
Multiply those stats by two and one can begin to get a measure on the danger of intubating an individual suffering from Covid-19. The virus invades the lungs, changing their composition from its usual rich, oxygen-transferring alveoli to drenched fluid sacs incapable of transferring oxygen from the air we intake into oxygen the blood needs to maintain life functions. A ventilator forces pressured air into the lungs – pressure which stresses the already-damaged alveoli and has already cause ruptures in lung tissue leading to death.
I contrast the headlong preoccupation with air-ventilating Covid-19 patients in the US – most of whom die from the ventilation – with the measured and logical approach given Prime Minister Boris Johnson in London, where he was administered oxygen via face mask and seems to be recovering steadily with no side effects.
Air is only 21% oxygen. Why force pressured air down the weakened lungs of a Covid patient when it’s not 78% nitrogen that’s needed? It’s oxygen!! And the danger of bursting lung tissue is obviated. Seems elementary.